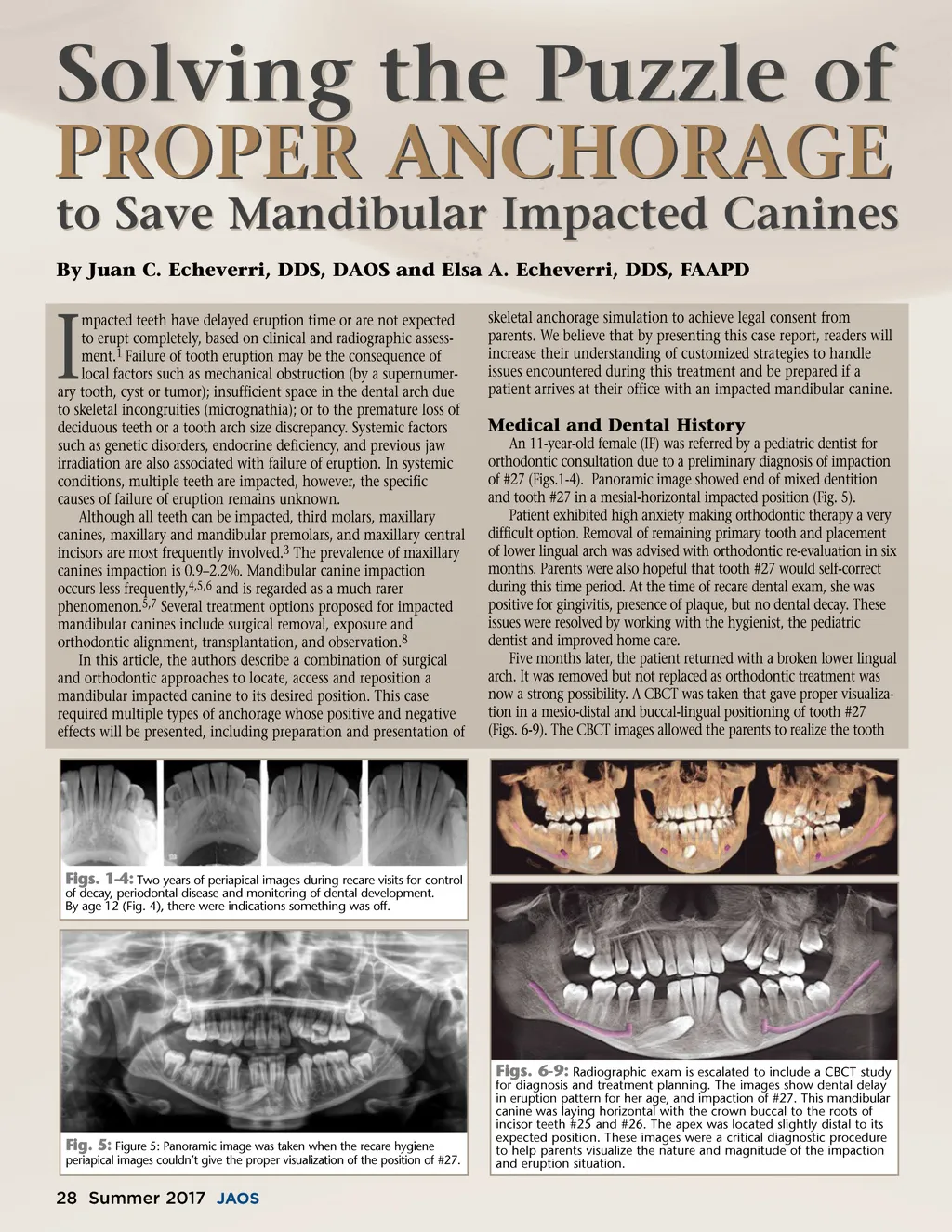
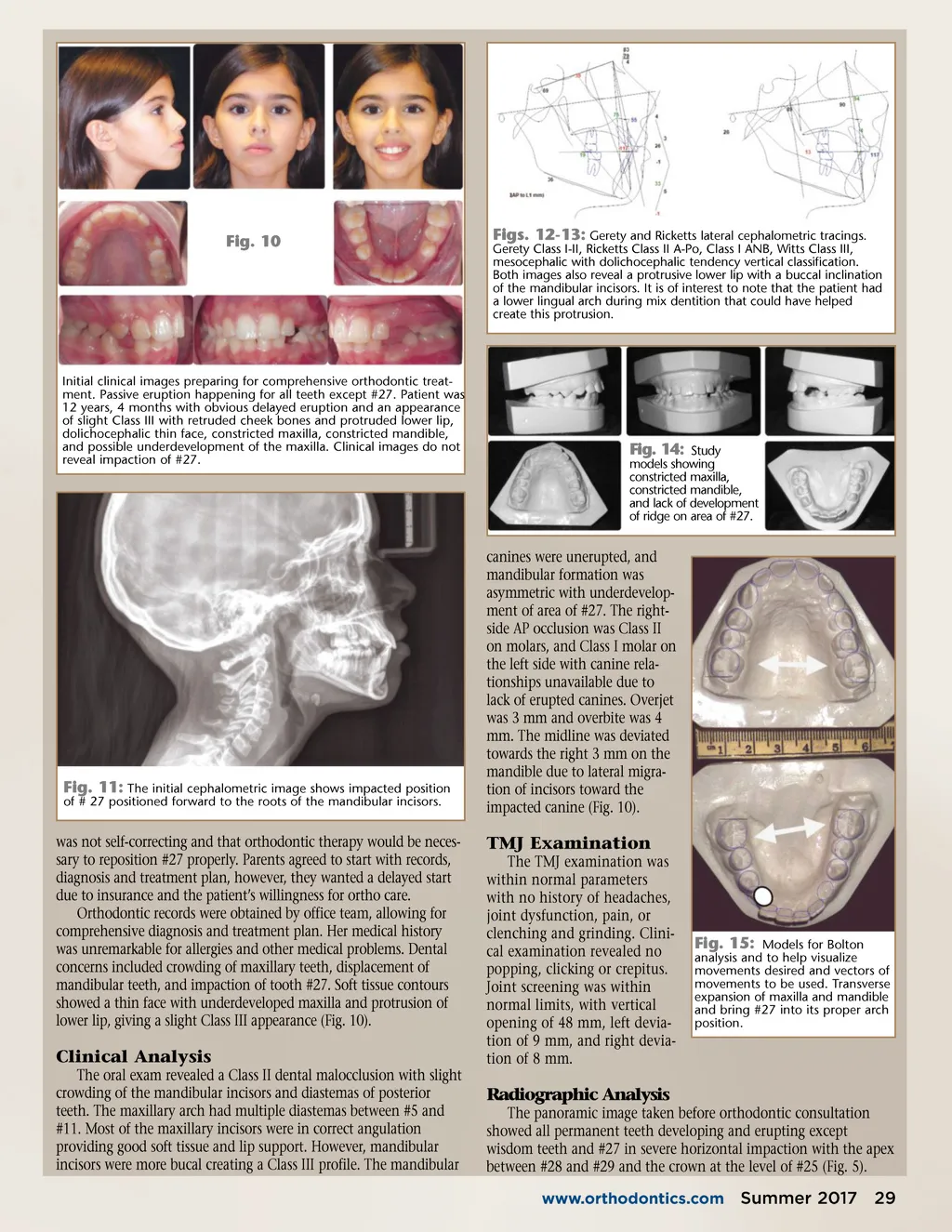
PROPER ANCHORAGE By Juan C. Echeverri, DDS, DAOS and Elsa A. Echeverri, DDS, FAAPD Solving the Puzzle of to Save Mandibular Impacted Canines mpacted teeth have delayed eruption time or are not expected to erupt completely, based on clinical and radiographic assess-ment. 1 Failure of tooth eruption may be the consequence of local factors such as mechanical obstruction (by a supernumer-ary tooth, cyst or tumor); insufficient space in the dental arch due to skeletal incongruities (micrognathia); or to the premature loss of deciduous teeth or a tooth arch size discrepancy. Systemic factors such as genetic disorders, endocrine deficiency, and previous jaw irradiation are also associated with failure of eruption. In systemic conditions, multiple teeth are impacted, however, the specific causes of failure of eruption remains unknown. Although all teeth can be impacted, third molars, maxillary canines, maxillary and mandibular premolars, and maxillary central incisors are most frequently involved. 3 The prevalence of maxillary canines impaction is 0.9–2.2%. Mandibular canine impaction occurs less frequently, 4,5,6 and is regarded as a much rarer phenomenon. 5,7 Several treatment options proposed for impacted mandibular canines include surgical removal, exposure and orthodontic alignment, transplantation, and observation. 8 In this article, the authors describe a combination of surgical and orthodontic approaches to locate, access and reposition a mandibular impacted canine to its desired position. This case required multiple types of anchorage whose positive and negative effects will be presented, including preparation and presentation of skeletal anchorage simulation to achieve legal consent from parents. We believe that by presenting this case report, readers will increase their understanding of customized strategies to handle issues encountered during this treatment and be prepared if a patient arrives at their office with an impacted mandibular canine. I Medical and Dental History An 11-year-old female (IF) was referred by a pediatric dentist for orthodontic consultation due to a preliminary diagnosis of impaction of #27 (Figs.1-4). Panoramic image showed end of mixed dentition and tooth #27 in a mesial-horizontal impacted position (Fig. 5). Patient exhibited high anxiety making orthodontic therapy a very difficult option. Removal of remaining primary tooth and placement of lower lingual arch was advised with orthodontic re-evaluation in six months. Parents were also hopeful that tooth #27 would self-correct during this time period. At the time of recare dental exam, she was positive for gingivitis, presence of plaque, but no dental decay. These issues were resolved by working with the hygienist, the pediatric dentist and improved home care. Five months later, the patient returned with a broken lower lingual arch. It was removed but not replaced as orthodontic treatment was now a strong possibility. A CBCT was taken that gave proper visualiza-tion in a mesio-distal and buccal-lingual positioning of tooth #27 (Figs. 6-9). The CBCT images allowed the parents to realize the tooth Figs. 1-4: Two years of periapical images during recare visits for control of decay, periodontal disease and monitoring of dental development. By age 12 (Fig. 4), there were indications something was off. Fig. 5: Figure 5: Panoramic image was taken when the recare hygiene periapical images couldn’t give the proper visualization of the position of #27. Figs. 6-9: Radiographic exam is escalated to include a CBCT study for diagnosis and treatment planning. The images show dental delay in eruption pattern for her age, and impaction of #27. This mandibular canine was laying horizontal with the crown buccal to the roots of incisor teeth #25 and #26. The apex was located slightly distal to its expected position. These images were a critical diagnostic procedure to help parents visualize the nature and magnitude of the impaction and eruption situation. 28 Summer 2017 JAOS
Journal of the American Orthodontic Society Summer 2017/Buyer's Guide: Page 28